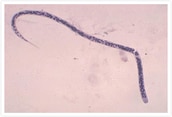
Onchocerciasis, or river blindness, is an infectious disease caused by the parasitic worm Onchocerca volvulus. It is transmitted through repeated bites by black flies of the genus Simulium. Adult worms live in fibrous nodules under the skin. An infection causes intense itching and other symptoms. When it progresses, O. volvulus microfilariae concentrate on eyeballs that can lead to eye disease resulting in blindness. Along with trachoma, onchocerciasis is one of the world’s leading causes of preventable blindness.
Causes of Infection
Onchocerciasis is caused by the helminth Onchocerca volvulus. Also known as river blindness, it is an infectious disease that is transmitted from person to person by the black fly. When a black fly bites an infected patient, larvae known as microfilariae that live in the patient’s skin enters the body of the fly, infecting it with the parasite in turn. The microfilariae then develop in the fly to a stage where the worms are again infectious to humans, thus continuing a cycle of infection. The name “river blindness” derives from the fact that the infected black flies tend to live and breed near rivers or streams where the water flows at a relatively rapid rate and that the disease can often lead to blindness.
The larvae develop over two weeks in the fly to a stage that is infectious to humans. The infective larvae, which have moved to the female black fly’s head or proboscis, enter human body when the fly bites to suck blood. Once inside a human body, the larvae mature into adults in around three months to one year. Most adult worms live in fibrous nodules under the skin and sometimes near muscles and joints.
Disease Agent:Parasitic worm Onchocerca volvulus
Vector:Black flies of the genus Simulium

Symptoms
The infection causes intense itching, nodules under the skin with changes in skin color, and eye disease leading to blindness; these are the three distinctive symptoms of onchocerciasis. Furthermore, the lymph glands of infected patients have been observed to swell up in some cases, but this is non-painful and relatively uncommon.
It can take up to one year for the larvae to develop into adults inside the human body and some of the infected do not show any early symptoms. An adult female worm, which can live from 10–15 years, can produce millions of microfilariae during its lifetime. Most patients infected with this disease, however, will normally continue to feel well until the large numbers of larvae are produced even if adult worms are already present in the body, as onchocerciasis symptoms are mainly caused by the microfilariae themselves.
Specifically, the majority of symptoms develop due to responses from the patient’s body to dead or dying populations of microfilariae. For example, skin inflammation not only causes itching but also long-term damage such as changes in skin tone that can result in a “leopard-print” appearance as well as thinning skin, through which a resulting loss of elasticity can lead to an appearance that is sometimes described as resembling “cigarette-paper.” Furthermore, if microfilariae die within or in the vicinity of the eye, reversible lesions on the cornea without treatment in the early stages can progress to permanent corneal clouding and eventually blindness. Inflammation of the optic nerve has also been observed to lead to vision loss, particularly in terms of peripheral vision, and eventual blindness in untreated patients.
Onchocerciasis is one of the world’s leading causes of preventable blindness. Along with trachoma, it is known as an infectious disease that can cause blindness.
Diagnosis and Treatment
Diagnostic Methods
The diagnostic methods used today include:
Skin Snip
This is the most commonly used approach to diagnosing for the disease. In this method, a 1 to 2 mm shaving or biopsy of the skin is performed to confirm the presence of the larvae, as larvae will typically protude from the skin’s surface when immersed in normal saline or other physiologic solutions. Usually, six snips are taken from different areas of the body, including the iliac horn, scapula, and lower limbs. Polymerase chain reaction (PCR) of the skin can be used for diagnosis if larvae are not seen.
Antibody Test
Antibody tests can often detect early-stage infections. Since such tests are unable to distinguish between previous and current infections, however, they are not as effective for people who live or have lived in an endemic area. Antibody tests are considered effective for diagnosing for the disease in visitors to an endemic area.
When infection with the disease is strongly suspected on clinical grounds, antibody test results, even in cases where a skin snip test has indicated a negative, should only be used as provisional criteria for arriving at a final diagnosis. Similarly, if the test results in a positive, both additional antibody tests and additional skin snip tests are recommended before a conclusive diagnosis can be made.
Polymerase Chain Reaction (PCR)
When larvae are too few to be spotted, polymerase chain reaction (PCR) of the skin is applied. However, this test is usually conducted in a laboratory and it is not easily done at the place of infection.
Slit-Lamp Examination
Infections in the eye can be diagnosed with a slit-lamp examination of the anterior part of the eye, where the microfilariae or the lesions that they cause are visible.
Treatment
Two types of oral drugs, ivermectin and doxycycline, are used to treat onchocerciasis.
Ivermectin
This agent has been demonstrated to decrease instances of blindness and lower the frequency and severity of skin-related symptoms. One dose of ivermectin significantly decreases the microfilarial load that can last a year or more. Generally one dose of ivermectin is administered every three to six months while the symptoms remain visible. Ivermectin kills the microfilariae (larvae), but not the adult worms.
Doxycycline
One medicine that continues to evolve over time is doxycycline, which according to clinical studies has been shown to eradicate the rickettsia-like Wolbachia, a type of endosymbiotic bacterium. Daily treatment with a six-week course of doxycycline kills more than 60% of the adult female worms and sterilizes 80 to 90% of the females 20 months after treatment. On the other hand, doxycycline is not effective against microfilariae.
In patients with nodules in the skin, the nodules can be surgically removed and examined for adult worms.
Prevention
Currently, there is neither a vaccine nor a recommended drug available to prevent onchocerciasis. Since black flies bite during the day, the best prevention is to avoid being bitten by infected black flies by using insecticides that contain N,N-Diethyl-meta-toluamide (DEET) on exposed skin, wearing long-sleeved shirts and pants, and wearing clothing treated with permethrin.
Regions at High Risk of Infection
Onchocerciasis is often found in agrarian areas in tropical sub-Saharan Africa. According to data released in 2017 by WHO, 99% of those infected are concentrated in 31 countries in Africa. The remaining 1% are found in Yemen and among the Yanomami people living in Brazil and Venezuela.
Estimated Number of Infected People
According to data released by CDC in 2013, 123 million people are at risk of infection, with 25 million already infected globally.
Estimated Number of the Deaths
While onchocerciasis is rarely the direct cause of death, infection can result in blindness.
References
WHO- Neglected Tropical Diseases, accessed March 19, 2014,
http://www.who.int/neglected_diseases/mediacentre/factsheet/en/
CDC- Neglected Tropical Diseases, accessed March 19, 2014,
http://www.cdc.gov/globalhealth/ntd/diseases/